
History taking
1) When do you notice the ulcer?
Remember that the ulcer might have been present for long before the patient actually notices it. This is usually in case of a neuropathic ulcer.
2) What draws your attention to the ulcer?
Usually is because of pain. Others includes : bleeding, discharge, may be foul-smelling.
3) How does the ulcer disturbs you?
The commonest symptom associated with an ulcer is pain. It might be interfering with eating, walking, defecating, etc
4) Any changes to the ulcer since you've noticed it?
Is there any increase in size, changes in shape, increased discharge, bleeding, or severity of pain?
5) Is there any similar ulcers noticed elsewhere in the body?
Asking for multiplicity.
6) What do you think is the cause of ulcer?
Most of the time the patient will get it right, and the commonest cause is trauma.
Examination
1) Inspect the floor
The floor of an ulcer usually made up of granulation tissues or slough tissues. Sometimes, the underlying structures might been exposed, eg : bones, tendons, etc. Some characteristic contents of the floor are able to provide you a hint to your diagnosis :
Solid-Brown, greyish tissue - Full thickness death of tissue
Slough tissue resembles a yellow-grey wash leather - Syphilitic ulcers
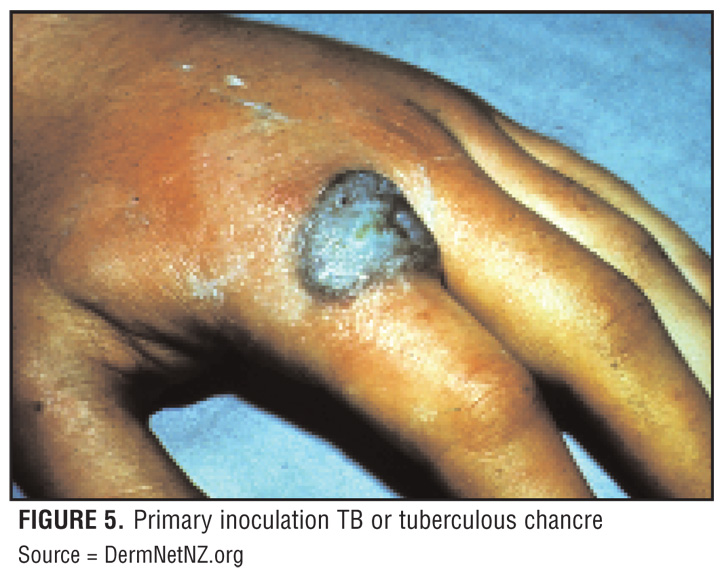
Unhealthy, bluish granulation tissue - Tuberculous ulcers
Poor granulation tissue, with visible bones, tendons, periosteum - Ischaemic ulcer
2) Edge of the ulcer
The edge is the portion in between the floor and margin of an ulcer
There're 5 main types of edges for ulcer :
a) Slopping edge
Usually means the ulcer is superficial/shallow and has a good chance in healing. Healthy granulation tissue usually is pinkish, means it has a good vascularity. A healing epidermis is usually seen extending from the edge, over granulation tissue, either pale/pink in colour (almost transparent)
One example of such ulcer is - venous ulcer

It means there's rapid death over full thickness of tissue with minimal attempts of the body to repair it. A classical textbook example is the Ulcers seen in tertiary syphilis. Nowadays, ulcers with punch out edges are more commonly seen in neuropathic or peripheral arterial ischaemic ulcers. (PVD)

c) Undermined edge
It means the rate of destruction of the subcutaneous tissue is more rapid than the skin, causing the edge of ulcer to be undermined. Classical example, as it's rarely seen nowadays is tuberculous ulcers. Ulcers with undermined edge is more commonly seen in bedsores, pressure sores as the subcutaneous tissues are more susceptible towards pressure.

d) Everted edges

This means that over the edges of the ulcer, tissues are growing so rapid that it eventually overlaps the overlying skin. This is classically seen in Squamous cell carcinoma.
e) Rolled edges

The tissues over edges are growing slowly, which is usually pale/pink in colour, with telengiectasis seen over the pearly edges. An ulcer with rolled edges is almost diagnostic of a rodent ulcer of Basal cell carcinoma.
3) Depth
Measure the depth of an ulcer by mm
4) Discharge
Discharge from an ulcer can be serous, serosanginous, sanginous, or purulent.
Sometimes, due to the formation of a coagulation discharge scab over an ulcer, it prevents you from examining the entire structure of ulcer (might be missing some of it's features). It's advised that you remove the scab first.
5) Base
Feel the base of the ulcer.
Is it adherent to the underlying structure? (may be bone, periosteum, tendon in cases of osteomyelitis, malignancy)
6) Regional lymph nodes
Please remember to palpate the regional lymph nodes.
It'll be enlarged (and tender) if there's secondary metastatic deposits or any spreading infection.
7) State of the local tissues
Most of the ulcers over the leg is due to poor vascular/nervous supply.
Hence, it's a must that you check for it's vascularity and innervation.
helpful... worth reading
ReplyDeletePERMANENT DOCTOR NEEDED - URGENT !!!
ReplyDeleteWe are Owner and Operator a General Practice (GP) Clinic in Bandar Sungai Long, Bangi and Putrajaya (Presint Diplomatik - Klinik Pakar KASIH).
We are looking for a dedicated Medical Officer Requirements at Bandar Sungai Long Clinic:-
Lady doctor
MBBS or equivalent from a recognized institution approved by Ministry of Health Malaysia
Possess valid Annual Practicing Certificate
Registered with Malaysia Medical Council
Minimum 2 years working experience in Obstetric & Gynecology
Attended an Obstetric Life Saving Skill
Attended A Neonatal Resuscitation Program
Working hours negotiable with minimum on-call
Very attractive salary RM7,000 (starting)
Kindly please send to recommend CV to: aznial@gmail.com
Clinic information:-
PUSAT RAWATAN SUNGAI LONG
NO. 12 JALAN SL 1/13
BANDAR SUNGAI LONG
43000 KAJANG
SELANGOR
TEL / FAX: 03-90114833