
Almost all cases of Bladder carcinomas are originating from the transitional epithelium.
Since, the urothelium is frequently exposed to carcinogens that might be excreted through the urine. Urothelium over the bladder is commonly involved since there's always residual urine.
Occasionally, bladder carcinoma might be squamous cell in nature.
This is usually seen when there's chronic inflammation of the bladder mucosa, caused by stones or schistosomiasis.
Rarely, it presents as adenocarcinoma.
Usually due to local infiltration of tumour from pelvic organs, or bowel.
History and examination
Males are 3 times more likely to have CA bladder than females.
Age of presentation is usually around 60-70s.
Certain occupations are at high risk of developing this malignancy, especially those frequently deals with chemical dyes (Naphthylamine and Benzidine):
Leather workers
Painters or decorators
Paper or rubber manufactures
Dental technicians
Painless and terminal or total hematuria present in about 80% of the cases
Sometimes, patients might be passing out blood clots
Hence, there might be dysuria, or difficulty in micturition
If the residual urine gets infected, there's symptoms of cystitis
If the tumours originating from the ureteric orifice of bladder, loin pain can present
If infiltration had taken place to adjacent structures, lower abdominal pain radiating to the legs might be present
Bear in mind that for patients with recurrent cystitis not responding to treatment, think of CA bladder.
On examination, usually is not very helpful.
Mass may be palpable over the suprapubic area, over even during per rectal examination.
TMN staging of bladder carcinoma

Tis - Carcinoma in situ, means tumour cells are present only over the inner lining
Ta - Non-invasive, papillary tumour
T1 - Invasive, however, yet to involve the bladder musculature
T2a and T2b - Infiltration beyond bladder musculature
T3a and T3b - Infiltration into the fatty tissue around the bladder
T4a and T4b - Invasion into the adjacent organs (prostate, pelvic wall)
Investigation
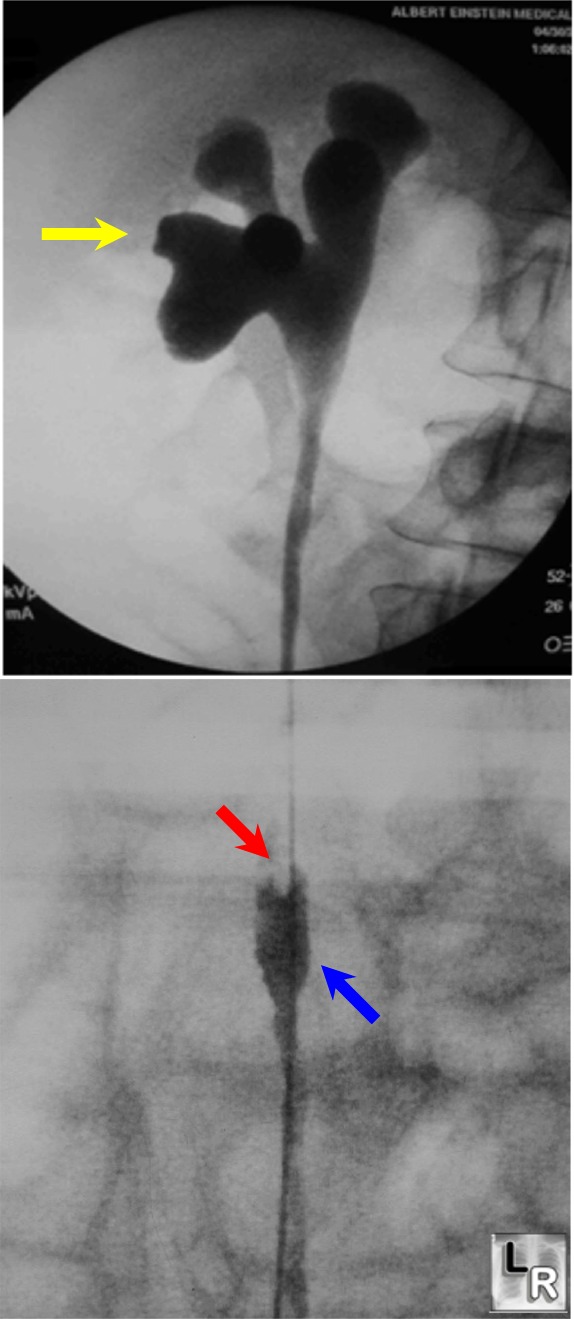
Intravenous urogram will shows filling defect within bladder :

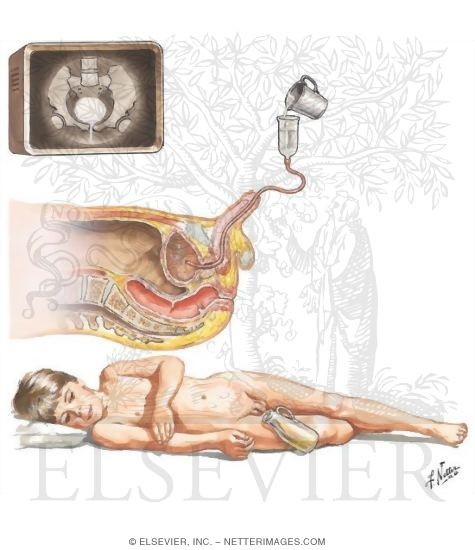
IF such picture is seen, a retrograde ureteropyelogram is indicated
Then, cystourethrography should be done under general anasthesia for examination of the tumour, and biopsy specimen can be taken.
CT abdomen for staging.
No comments:
Post a Comment