
The portal vein is formed behind the neck of pancreas, at the level of L2, by the superior mesenteric and splenic veins.
It ascends up along the free edge of lesser omentum, behind the common bile duct.
It enters the liver by dividing into two of it's tributaries.
The left and right gastric veins joins to it.
The inferior mesenteric veins drains into the splenic veins.
Portal vein is valveless and hence, if there's a raised in pressure in between the right heart and the splanchnic circulation, portal pressure elevates.
The portal vein carries about 1.5L of blood per minute, originating from :
Small bowel (superior mesenteric vein)
Large bowel (inferior mesenteric vein)
Spleen (Splenic vein)
Gastric vein
Pathophysiology
Normal portal pressure is about 5-10mmHg.
Portal hypertension occurs when the portal pressure elevates beyond 12mmHg.
At this point, the collaterals at sites of porto-systemic anastomosis opens up in order to decompress the elevated pressure in the portal system.
As the portal pressure elevates above 20mmHg, there's a risk of the friable, submucosal esophageal varices to rupture, causing massive hematemesis.
Sites of porto-systemic anastomosis :

2) Caput medusae : Paraumbilical veins (systemic) and vein within the ligamentum teres (portal)
3) Lower rectum : Superior and middle haemorrhoidal veins (portal) and inferior haemorrhoidal veins (systemic)
4) Perihepatic veins of Sappey : Subdiagphramatic veins (portal) and Veins at the upper surface of right liver lobe (systemic)
5) Retroperitoneal veins of Retzius : Retroperitoneal veins (systemic) and Superior + Inferior mesenteric veins (portal)
Causes :
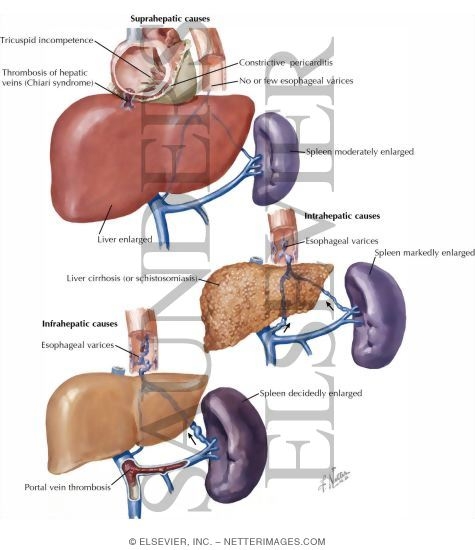
Portal vein thrombosis - seen in umbilical sepsis (infants)
Splenic vein thrombosis - Complication of pancreatitis, pancreatic tumour
b) Intrahepatic Causes :
i) Pre-sinusoidal :
Schistosomiasis
Primary biliary cirrhosis
Chronic active hepatitis
Sarcoidosis
ii) Sinusoidal :
Cirrhosis
Cytotoxic drugs
Vitamin A intoxication
iii) Post-sinusoidal :
Cirrhosis
Veno-occlusive diseases
c) Post-hepatic causes :
Budd-Chiari's syndrome
Tricuspid regurgitation
Constrictive Pericarditis
Clinical presentation (History and Examination)
Malnutrition
Ascites
Hematemesis and Malena
Encephalopathy
Caput medusae
Splenomegaly
Venous hum heard
Look for signs and symptoms of chronic liver disease
How do you manage these patients?
1) Esophageal varices without prior h/o of bleeding
Medical management is ideal in such cases.
Start Propanolol orally to reduce portal pressure, provided that there's no contraindication against B-blockers.
If contraindication present, isosorbide-5-mononitrate is an alternative.
Studies have shown that B-blockers reduces 45% of the risk of bleeding.
2) Ruptured esophageal varices presented with hematemesis
95% of the cases - originating from the esophageal varices, 5% - gastric origin
First, assess the rate and volume of bleeding :
Take pulse and BP in standing and sitting position
Gain IV ascess - Blood is withdrawn for hematocrit, coagulation profile, LFT and BUSE, blood grouping and cross matching
Provide immediate fluid resuscitation (Crystalloids, colloids, or even blood transfusion)
Insert CVP line - for ease of rapid transfusion later to prevent volume overload

Start Vasopressin IV (Contraindicated in angina) or Somastostatin IV.
Or Octreotide IV (more potent and duration of action is longer)
Usually 3 days later, as the patient's condition has stabilised, start B-blocker to reduce portal pressure and prevent further bleeding.
Plan for endoscopic treatment :
a) Band ligation
b) Sclerotherapy (Sodium Tetradecyl Sulphate - STS)
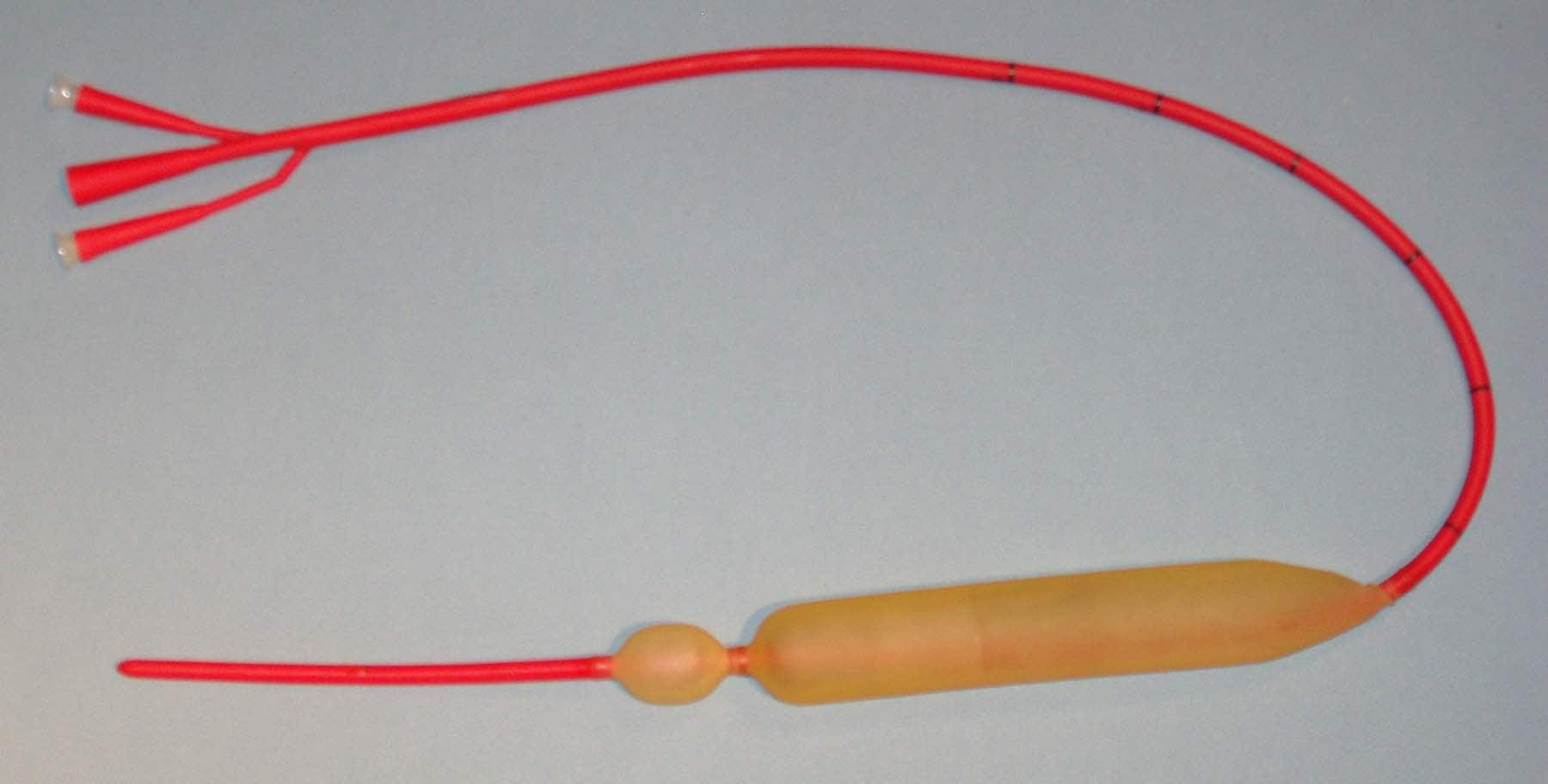
If the patient is not reponsive to the above measures and still bleeding or endoscopic intervention is not available (district hospitals), a Sangstaken-Blakemore tube can be inserted to prevent bleeding to buy time for deciding what's the next step. (Shoiuld be removed after 48 hrs)

Start oral neomycin (to reduce bowel flora -> less conversion of nitrogenous waste within bowel back to ammonia -> prevent hyperammonemia)
Start lactulose (to reduce bowel transit time)
Repeat every 2 weeks the sclerotherapy/band ligation until all the varices have been treated.
NICE BLOG!!! Thanks for your valuable information, It would be really helpful about Portal information Am working in Portal development company Bangalore .
ReplyDeleteI really appreciate sharing this great post. Keep up your work.Thanks for sharing this great article.Great information thanks a lot for the detailed article. That is very interesting I love reading and I am always searching for informative information like this.
ReplyDeleteclinical portal
This was an extremely wonderful post.
ReplyDeletekilt hire dundee keith scott
thomas doucet bagpipes
rg hardie
house of henderson kilts
kilt jackets aberdeen
kilt rental portland oregon
keith scott dundee
murray bagpipes
scotland trading company
gilt edged kilt hire glasgow
You can do very creative work in a particular field. Exceptional concept That was incredible share.
ReplyDeleteOakland A's Starter Jacket
FON PERDE MODELLERİ
ReplyDeletenumara onay
mobil ödeme bozdurma
NFTNASİLALİNİR
Ankara evden eve nakliyat
TRAFİK SİGORTASİ
dedektör
KURMA WEB SİTESİ
ask kitaplari
SMM PANEL
ReplyDeleteSMM PANEL
iş ilanları
instagram takipçi satın al
hirdavatciburada.com
beyazesyateknikservisi.com.tr
servis
tiktok jeton hilesi
nft nasıl alınır
ReplyDeleteen son çıkan perde modelleri
minecraft premium
yurtdışı kargo
en son çıkan perde modelleri
uc satın al
özel ambulans
lisans satın al
https://charlidameliomerch.shop/You can do very creative work in a particular field. Exceptional concept That was incredible share
ReplyDeleteThanks for sharing this premium article.
ReplyDeletehttps://themobileprices.pk/oppo-a15-price-in-pakistan/
The data you have posted is extremely helpful. chromeheartsoutfit
ReplyDeleteI am very happy to see this post. I found the most beautiful material fmerchandise I am very glad to visit your post.
ReplyDeleteThis is a great inspiring article.I am pretty much pleased with your good work. You put really very helpful information. Keep it up. Keep blogging. Looking to reading your next post.안양출장샵추천
ReplyDelete부천출장샵추천
광명출장샵추천
동두천출장샵추천
평택출장샵추천
안산출장샵추천
고양출장샵추천
과천출장샵추천
This post is good enough to make somebody understand this amazing thing, and I’m sure everyone will appreciate this interesting things. If you are a students and looking for assignments on corporate taxes then you can visit: Corporate Taxes Assignment Help.
ReplyDelete