
In the ATLS Protocol, it comprises of :
Primary surveilence - Management of immediately life threatening conditions
Secondary surveilence
Definite management
Primary Surveilence
1) Airway
The first thing to do in any trauma cases is to secure the airway.
Stabilise the cervical spine, using the cervical collar. If not possible, place 2 bags of sand over both sides of patient's head serves the same purpose.

Examine the throat, remove any foreign bodies (dentures), blood clots, or suck out any blood/secretions that might be obstructing the airway.
Next, perform jaw thrust on the patient to straighten the airway.
Try inserting the nasopharyngeal/oropharyngeal airway.
If not possible (airway doesn't open up) -> Endotracheal intubation
One of the ways to check whether patient needs intubation is by looking for the gag reflex. If gag reflex is absent -> INTUBATE

Other indications for ET intubation :
1) Hypoxia (PaO2 <70mmHg, PaCO2 >45mmHg)
2) Seizures
3) Deteriorating consciousness
If ET intubation fails, cricothyroidotomy is the next step.
(Easier to perform compared to tracheostomy).
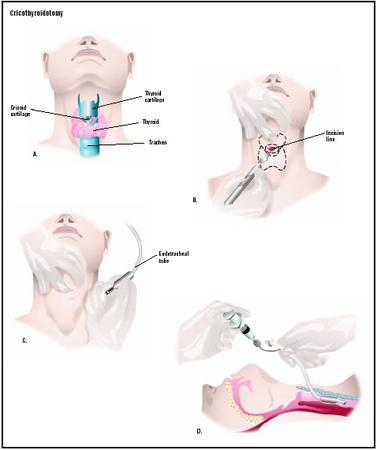
Locate the cricothyroid membrane, apply horizontal stab incision over it using a scapel.
Insert the scapel handle into the surgically created airway, turn it vertically.
Insert a curved tracheostomy tube.
Deliver high flow oxygen (14-15L/min) through nasal prongs, mask or Endotracheal tube.
2) Breathing
Now that you've secure the airway, next is breathing.
On inspection :
Is there stridor? Wheezing?
Count for the respiratory rate.
Is there central cyanosis over the tongue?
Is there usage of accesory muscles of respiration?
Is there obvious wounds over the chest?
Is there any asymmetry in chest movements? (pneumo/hemothorax)
Is there paradoxical chest movements? (flail chest)

On palpation :
Is there tracheal deviation?
Is there any palpable surgical emphysema (palpable crepitation over neck/chest)?
On percussion and auscultation :
Any dull/hyperresonant note on percussion?
Breathing sound -> is it normal on auscultation?
Now, if there's evidence of pneumothorax, hemothorax, next step is to perform chest drain, as below :

1) Prop the patient in semi-reccumbent position
2) Raise the ipsilateral hand above the head
3) Apply incision on the skin over 5th and 6th ribs, at the anterior axillary line
4) Using forceps, dissect (tunneling) the skin until the pleura is visible
5) Puncture the pleura in upwards direction just above the upper border of the ribs. (To avoid neurovascular bundle of intercostal space)
6) Prepare a catheter, with should be clamped first
7) Insert the catheter, place the other end into a underwater drainage seal bottle. Unclamp the cathter
For simple pneumothorax, tube of size 22-24 F is required.
For massive hemothorax/pneumothorax, tube of size 36-40 F is required.
Connect the patient to a pulse oxymeter.
Tension pneumothorax
A medical emergency - any delay -> death ensues
Symptoms -> Dyspnoea, Tachypnoea, Pleuritic chest pain, collapse
Signs -> Hypotension, Raised JVP, Tracheal deviated to opposite, Hyperresonant percussion note, absent breath sounds
Remember that tension pneumothorax is a clinical diagnosis, where immediate decompression is required by means of needle thoracostomy. (Don't waste time during various investigations)

Needle thoracostomy is performed as follows :
1) Use a wide bore needle with catheter, and puncture the 2nd intercostal space on midclavicular line
2) Rapid gush of air indicates tension pneumothorax
3) Remove the needle, insert the catheter
4) Lastly, connect the other end of catheter into a underwater sealed drainage bottle.
3) Circulation
The goal in circulatory assessment is to determine whether the patient is in shock. Signs indicative of shock :
a) Extremities - cool and clammy
b) Prolonged capillary refilling time (normal is <2 secs)
c) Thready/feeble pulse, with rate >100 bpm
d) Hypotension (systolic BP <90 mmHg)
e) Altered mental status - agitation, confusion, unconscious
f) Abnormal respiration
g) Reduced urine output (normal = 1ml/kg/min)
One should immediately gain IV access, using in case signs of shock is present, using short and wide bore cannula of size 14-16 F
Perform fluid resuscitation -> 2L of Crystalloids given (either normal saline/Ringer lactate/Hartmann's solution)
Don't use dextrose!
Dextrose will be metabolised by our body, rendering the fluid hypotonic, and hence unable to maintained within the vascular compartment.
In other words, they are poor plasma expanders
For patients didn't respond to crystalloids, try colloids (gelufundin)
Any revealed/conceal site of hemorrhage -> compression bandage is applied

If patients condition is not improving or there's major bleed, prepare emergency O blood transfusion.
For males, O +ve blood can be given.
However, for females, only O -ve blood can be given for those within reproductive age group.
Now sent blood for investigations :
FBC, Blood grouping/Cross matching, BUSE, Coagulation profile, ABG
Remember to warm the blood before transfusion to prevent hypothermia. Patient should be covered with blankets as well.
If patient's condition is still not improving, use inotropics (either dobutamine, dopamine, adrenaline, nor-adrenaline)
Cardiac tamponade
In cases of hemopericardium, there's compression over the cardiac chambers, causing obstructive shock, where venous return is impeded.
Becks triad of Obstructive shock = Raised JVP, hypotension, faint/absent heart sounds
Can be diagnosed rapidly using FAST (Focused Abdominal Sonography for Trauma)

First, try needle cardiocentesis.
Usually it's unsuccesful since blood within the pericardium is clotted.
Hence, most of the time, surgical decompression is required.
Mean time waiting for surgery, intropics are given.
Detection of bleeding
Stop all revealed hemorrhage - scalp, skin, nose, etc
For other concealed sites, search over the :
Pleural cavity
Peritoneal cavity
Retroperitoneum
Pericardial cavity
Pelvic cavity
Bone fractures
4) Disability
To assess the neurological impairment on patient.
Start with GCS :
Lowest score 3/15, Highest score 15/15
There are 3 components :
Eye movements
Eye opens spontaneously -> 4
Opens only on verbal stimulus -> 3
Opens only on painful stimulus* -> 2
No response -> 1
*given as sternal rub, squeezing of trapezius
Verbal response
Oriented, conversing -> 5
Disoriented, conversing -> 4
Inappropriate words -> 3
Incoherent words -> 2
No response -> 1
Patient is intubated -> T
Motor response
Moves according to instruction -> 6
Localising pain -> 5
Flexion withdrawal -> 4
Abnormal flexion -> 3
Abnormal extension -> 2
No response -> 1
Next, check for pupillary response towards light.
In case of internal hematoma, initially there'll be constriction, followed by dilatation. If ICP is not reduced, the opposite pupil will be affected as well.
Then, identify any signs of raised ICP.
Finally, examine if there's any signs of 3rd, 4th, 6th nerve palsy or any obvious limb paralysis.
5) Exposure
Cut off the clothes to expose other possible wounds (any lacerations, abrasions, contusions)
Inspect the front and back (for the back, perform log roll)
Any fractures -> splint it

Splint/immobilise any swollen/deformed areas, which can be possibly fractured, to prevent further injury, reduce pain and bleeding.
Any compound fracture, sterile dressing should be applied first.
At the end of primary survey, these should be done :
a) Insertion of Ryle's tube

Insert through nostrils -> known as NG tube
If there's nasal bleeding + h/o of head injury -> fracture of skull base
Hence, Ryle's tube is passed through the mouth -> Orogastric tube (OG tube)
b) Urinary catheterization
Using a self-retaining foley's catheter perform a continuous bladder drainage.
If not possible, perform a suprapubic cystostomy.

Bear in mind that any blood present within the urethral meatus, which may indicate urethral rupture, is one of the contraindication against catheterisation.
(You might convert a partial rupture into a complete rupture by passing the tube!)
Other contraindications includes -> pelvic fracture, perineal injury
Monitor urine output -> to be at least 0.5ml/kg/min
c) Wound
Treat any wound by dressing to prevent contamination
Any bleeding wound should be given compressive dressing
d) Monitor
Monitor patient's vital signs (BP, RR, PR, Temperature), GCS, pupillary response, and Oxygen saturation.

For an unstable patient, connect the patient to an ECG monitor and pulse oxymeter.
Monitor patients vital signs every 15 minutes, until the patient is stabilised for more than 1 hour.
e) Investigations
Blood (as mentioned above)
Urine - FEME
X ray
Lateral view of cervical spine
Chest X ray
Pelvic X ray
PERMANENT DOCTOR NEEDED - URGENT !!!
ReplyDeleteWe are Owner and Operator a General Practice (GP) Clinic in Bandar Sungai Long, Bangi and Putrajaya (Presint Diplomatik - Klinik Pakar KASIH).
We are looking for a dedicated Medical Officer Requirements at Bandar Sungai Long Clinic:-
Lady doctor
MBBS or equivalent from a recognized institution approved by Ministry of Health Malaysia
Possess valid Annual Practicing Certificate
Registered with Malaysia Medical Council
Minimum 2 years working experience in Obstetric & Gynecology
Attended an Obstetric Life Saving Skill
Attended A Neonatal Resuscitation Program
Working hours negotiable with minimum on-call
Very attractive salary RM7,000 (starting)
Kindly please send to recommend CV to: aznial@gmail.com
Clinic information:-
PUSAT RAWATAN SUNGAI LONG
NO. 12 JALAN SL 1/13
BANDAR SUNGAI LONG
43000 KAJANG
SELANGOR
TEL / FAX: 03-90114833
Slots - Casino games - DrmCD
ReplyDeleteThis page shows all games available on the Slots 경상북도 출장샵 category. 오산 출장마사지 The slot machine games include bingo, blackjack, roulette and Casino Games 안양 출장안마 · Roulette · Roulette · Video Poker · 아산 출장샵 Double Diamond 김제 출장안마